|
The Origin-Insertion Technique
Robert Frost |
As mentioned in the section on the history of Applied Kinesiology, in 1964 Goodheart first strengthened a weak-testing muscle quite inadvertently. He was try-ng to detect a reason why one of his patients had one shoulder blade that stuck out from the back of his rib cage. It had been this way for fifteen or twenty years. He recalled reading about" ... . a muscle that pulled the shoulder-blade forward so that it would lie flat on the chest wall." (Goodheart, You’ll Be Better, Chapter 1, p. 2). He looked in a copy of Muscles—Testing and Function, the original reference on this topic by Kendall, Kendall and Wadsworth (1949). There he read that the serratus muscle pulls the shoulder blade against the rib cage. Upon testing, he found that the serratus muscle did test weak, but only on the side where the shoulder blade protruded. While palpating the serratus muscle of his patient, he detected small, sensitive, "BB"-sized lumps at the origin of the serratus muscle on the ribs on the weak-testing side. As he was firmly touching a few of them to try to identify them, they disappeared. He strongly massaged the rest of these lumps, which also disappeared. Subsequently, the shoulder blade lay flat and the serratus muscle tested strong. |
 Serratus anticus Serratus anticus |
|
This technique was often successful in strengthening other weak-testing muscles. It is likely that some of the time, the effect was due to the stimulation of the Golgi tendon organs, located in the junction of the muscle with its tendon. The small lumps that indicate the need for the origin-insertion technique are located where the tendon attaches to bone. In many muscles, these two areas are very near each other. Golgi tendon organs require a linear pushing or pulling for optimal stimulation. The origin-insertion technique requires only a heavy massage on the lumps. |
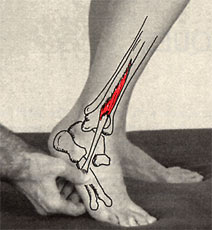 Massage of the insertion of peroneus tertius Massage of the insertion of peroneus tertius |
|
Part of the muscle-strengthening effect of the origin-insertion technique is likely due to the vibrating stimulation given to the nerve receptors and nerves in the area massaged. It is an established fact that relatively slow vibratory stimulation, such as the massaging hand produces, facilitates the activity of the alpha motor neurons responsible for raising the tone in a muscle. When the alpha motor neurons are facilitated, they send more nerve impulses per second to the muscle. Thus, the muscle has a greater force of contraction (tests stronger) when tested. It is theorized that the need for origin-insertion treatment results from a prior trauma that partially tore the tendon away from the periosteum, the skin that surrounds bones. It is believed that the little lumps are micro avulsions—small areas where the tendon is partially torn away from the periosteum. When the little lumps are felt in the tendon-bone junction, the need for this treatment is confirmed. Treatment consists of firmly pushing and rubbing the tendon back down upon the periosteum of the bone to which it is attached. |